Data from the International Training and Education Center for Health (I-TECH) program in Malawi were presented during the 2023 Conference on Retroviruses and Opportunistic Infections (CROI). The annual conference took place in Seattle, WA, from 19-22 February 2023, and brought together researchers, academics, and experts to discuss and present on their scientific achievements and new research.
During the “Insights into Prevention and Treatment of HIV in Women and Children” oral abstract session that was held on 20 February 2023, representatives from I-TECH Malawi presented on recent HIV infection surveillance data in breastfeeding women in Malawi:
The Centers for Disease Control and Prevention also presented a poster during the poster session that used data from the I-TECH Malawi HIV Recency Surveillance project:
The Alto Maé Reference Center (CRAM). Photo courtesy of I-TECH Mozambique.
Four decades into the HIV epidemic, more than 50,000 people per year in Mozambique continue to die from HIV-related conditions.
The Alto Maé Reference Center (CRAM) provides a specialized package of care and treatment services for patients with advanced HIV disease from the urban health network of Maputo, Mozambique. Since January 1, 2021, the International Training and Education Center for Health (I-TECH) has served as the Ministry of Health’s primary partner for managing CRAM, a role handed over by Médecins Sans Frontières (MSF), which established the clinic in 2010.
Since I-TECH started its activities at CRAM, the center has had 1,599 active patients in follow-up care.
“More than 80% of patients admitted to CRAM for specialized care are referred by other health centers,” explains Dr. Florindo Mudender, Country Director for I-TECH Mozambique. “Critically ill patients are treated at CRAM until they are stable, then sent back to their facilities of origin to continue treatment. In addition to acute care, CRAM also provides individualized supportive services to patients who often present with dire psychological, social, and economic conditions.”
These supportive services proved crucial to Aisha,* a 43-year-old mother of five who had difficulty accepting her HIV status, believing that her church’s pastor had cured her disease through prayer.
Referred to CRAM five years ago with a diagnosis of Kaposi’s sarcoma, Aisha was prescribed second-line antiretroviral therapy (ART). However, after losing her job due to COVID-19, Aisha was subject to food insecurity, discrimination, social stigma, and physical, psychological, and financial abuse by her partner.
After routinely presenting a high viral load and suffering severe weight loss, Aisha’s care team at CRAM assumed she had not been taking her medication – possibly because of her religious beliefs and a lack of food. She was severely depressed, to the point of attempting suicide.
Worried about her condition, the team at CRAM enrolled Aisha in wraparound services, including behavioral psychotherapy, education in self-care and self-esteem, treatment adherence support, positive prevention, couple’s therapy and socio-family integration, group therapy with other patients with depression, and antidepressant medication.
After several months, Aisha’s last viral load test showed a result of “undetectable,” and her depressive symptoms abated. Thanks in part to the support from CRAM, Aisha is now adhering to her ART, has regained her self-esteem, is working again, and eats regular meals. Her partner tested HIV-negative and has learned to support her so that she feels valued and loved. Aisha attends psychotherapeutic sessions quarterly at the CRAM to monitor her psychological and social well-being.
“[My husband] helps me a lot, so I don’t forget to take my pills, and I am very happy about that and with the improvement I made with my health,” says Aisha. “Before, we were hungry, and now, I am back to work. With the little I earn I can help with the household expenses.”
CRAM is considered a center of excellence and the main training site for AHD for Mozambique Ministry of Health clinicians and PEPFAR-funded implementing partners.
“I-TECH is currently refining a referral and counter-referral system between CRAM and Maputo City’s health centers, to ensure patient care continues after discharge,” says Dr. Mudender “The system will include a free mobile line to assist clinicians with advice from senior specialists.”
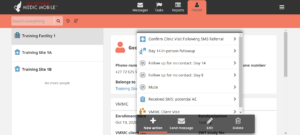
I-TECH, in close partnership with voluntary medical male circumcision (VMMC) implementing partner, the Aurum Institute and technology partner, Medic, is conducting a five-year study funded by the National Institutes of Health to further evidence on the efficiency, safety, and scalability of two-way text-based (2wT) follow-up for VMMC services.
2wT is SMS-based telehealth, providing direct patient to provider communication that improves the quality of post-operative VMMC care. A daily educational message is sent to each participant, requesting a response to report potential complications. 2wT allows the nurse to triage men to care when needed or desired while supporting most men to heal independently at home. 2wT-based follow-up dramatically reduces unnecessary post-operative visits, saving patient and provider costs, while improving patient care quality through swift identification and referral for potential adverse events. In South Africa, the 2wT intervention benefits were similar across routine VMMC programs in both rural and urban settings.
For nearly a decade I-TECH has worked in Côte d’Ivoire in collaboration with the US Centers for Disease Control and Prevention to develop and implement an electronic laboratory information system (LIS) in key laboratories. In order to respond to evolving data needs and ensure timely access to quality laboratory data, an electronic LIS requires ongoing development and continuous user training and technical support.
Previously, from 2015-2017 I-TECH worked closely with the Ivorian Ministry of Health and Public Hygiene (MSHP)’s Directorate of Informatics and Sanitary Information (DIIS) to identify, develop and reinforce the capacity of local professionals to lead and conduct LIS training, deployment, and maintenance activities in anticipation of national roll-out of the LIS at 96 general hospital laboratories. As part of this effort, and in collaboration with the DIIS, I-TECH trained users and deployed LIS at 13 national and regional level laboratories. Between 2013 and 2015, the total number of local professionals competent in LIS deployment increased to 24 local LIS support providers, while the number of in-country LIS trainers increased to 27. Within ten months, local IT providers and trainers trained over 75 health care workers to use an LIS and implemented an LIS at 36 laboratories. During supervision visits to 26 laboratories, within 4 to 6 months post-installation, 25 out of 26 (96%) of laboratories were actively using the LIS.
More recently, Côte d’Ivoire International Training and Education for Health (I-TECH CIV), I-TECH’s local partner in Côte d’Ivoire, has started working directly with CDC and DIIS and continued to engage I-TECH computer developers and deployment strategists to continue the progress with LIS.
I-TECH continues to make considerable progress with code base development for OpenELIS. For more information, visit the OpenELIS Global website.
“I-TECH prides itself on working collaboratively with our international partners. We held the principle from day one that the most successful programs happen when the locus of control sits in-country,” said Marrianne Holec, Senior Program Manager at I-TECH. “We had the foundation in place with our local staff, what was missing was the organizational structure to allow the team in-country to truly lead the project. With the formation of Zim-TTECH, I’m happy to say we are there.”
Among USG funders, it’s recognized that future models for sustainable healthcare rely on local country ownership and leadership.[1] But making the transition from US-based ownership to country ownership isn’t a one-time event, added Holec, “It’s a process that takes time. We wanted to document our process so that other international organizations who are looking to pursue decolonizing global health programming can learn from our experience.”
Through 16 key informant interviews, the team gathered views on transition planning, implementation, and technical support, ethics, and success. Five themes emerged from the data collected:
Develop a vision and empower leadership for change by delegating clear roles and supporting local ownership;
Plan and strategize for transition in a manner that accounts for historical context;
Communicate with and inform stakeholders to understand transition perceptions, understand barriers to transition, and enable open communications related to risks and benefits;
Engage and mobilize staff by constructing necessary infrastructure and providing technical assistance as needed; and
Define short-term and long-term success.
“Sustainability of successful donor funded public health programs is critical if we want to maintain the important gains that have been made over the years,” says Dr. Batsi Makunike, Executive Director of Zim-TTECH. “Strong local organizations with good governance, management, and technical capacities are an important cornerstone of sustainability.
“The process of transitioning from an international to a local organization is daunting,” she continues. “We hope that this study is helpful to other organizations in their efforts to transition.”
[1] Goosby E, Von Zinkernagel D, Holmes C, Haroz D, Walsh T. Raising the Bar: PEPFAR and New Paradigms for Global Health. JAIDS Journal of Acquired Immune Deficiency Syndromes. 2012;60.
The initiative, conducted in partnership with the U.S. Centers for Disease Control and Prevention (CDC) and the Faculty of Medicine and Pharmacy (FMP) of the Université d’État d’Haïti, aims to contribute to the strengthening of human resources in health, increasing the number of qualified clinicians in Haiti. The year-long training comprises theoretical and practical components; this cohort’s practica took place at seven different university hospitals and other health institutions around the country.
“Haiti faces a serious problem of shortage of human resources in health, due in part to the ‘brain drain’ abroad,” says Dr. Jean Guy Honoré, Executive Director of CHARESS. “In some health facilities located in remote parts of the country, there are no physicians, and patients are seen by nurses who sometimes have limited knowledge of the management of infectious pathologies. This training aims to improve the skills of these nurses.”
This aptly fits the vision of CHARESS, which is “to be the reference center, in terms of training, research and technical assistance, allowing populations to receive quality care, with humanity,” says Dr. Honoré. Two other cohorts of nurses have already started this specialized training.
Dr. Bernard Pierre, Dean of the FMP, expressed a wish to strengthen the collaboration between the FMP and CHARESS to extend similar specialized training to doctors — in particular, general practitioners.
I-TECH and its partners have been working in Haiti since 2006, delivering training, clinical mentoring, health information systems, and other health systems strengthening interventions.
Julianne Meisner
Julianne Meisner, PHD, MS, BVM&S, is an epidemiologist, veterinarian, and Assistant Professor in the Department of Global Health at the University of Washington (UW), researching issues related to One Health and pandemics. Her work focuses on human health at the human-animal-environment interface, with an emphasis on novel pathogen emergence, the human health effects of livestock keeping, and anticolonial approaches to global One Health research. She has many years of experience conducting linked human-animal research among livestock-keeping communities in sub-Saharan Africa, and strong teaching and research interests in epidemiologic methods and biostatistics, in particular spatial epidemiology and methods for drawing causal inference from observational studies. She holds her veterinary degree from the University of Edinburgh, and her MS and PhD in Epidemiology from UW.
Her current projects focus on novel virus emergence at high-risk human-animal interfaces in South America, Africa, and Asia, and the role of land use change in disease emergence; methods for modeling human-animal contact networks for more accurate modeling of disease transmission between animals and humans; the role of land tenure and land rights in human and animal health; and One Health surveillance system strengthening.
From left to right: Conrad Mitchell, Program Coordinator, I-TECH Trinidad; Belinda White, Clinical Psychologist, I-TECH Trinidad; Heather Rodney, Chairperson, NACC Secretariat; Ian Ramdahin, Permanent Secretary, NACC Secretariat; Dr. Omoye Imoisili, Senior Public Health Analyst, HRSA; Aliyah Abdul Wakil, Strategic Information, HRSA; Alana Lum Lock Cardinez, Program Advisor, I-TECH Trinidad; Misti McDowell, Program Director, I-TECH headquarters.
Recently, representatives from the International Training and Education Center for Health (I-TECH) met with health officials in Trinidad and Tobago to discuss potential areas of support for strengthening the national response to HIV and AIDS in the country.
The meeting attendees discussed strengthening advocacy for people living with HIV (PLHIV); psychosocial support for vulnerable PLHIV; and providing services at the intersection of HIV and AIDS and gender-based violence (GBV).
With support from the Health Resources and Services Administration (HRSA), I-TECH has worked in Trinidad and Tobago since 2009, collaborating with the Ministry of Health and other partners to focus on healthcare worker training and technical assistance to improve the quality of care for PLHIV.
“I’ve always been impressed with the team and activities in Trinidad and Tobago,” says Misti McDowell, I-TECH Program Director, “especially the integration of much-needed mental health services into the HIV program.”
The assessment “Strengthening Delivery and Oversight of Mental Health and Psychosocial Services for PLHIV in Trinidad and Tobago” was completed by I-TECH and shared with the National AIDS Coordinating Committee (NACC), in an effort to identify future areas of collaboration. One of the intended outcomes is the establishment of a technical working group of national stakeholders who will collaborate with I-TECH to craft a strategy for implementing all priority interventions.
“The findings of this assessment revealed that there is a tremendous need for improved mental health support specifically in the areas of assessment and treatment throughout the national HIV treatment and care sites,” says Belinda White, Clinical Psychologist with I-TECH. “One treatment and care site reported that as much as 90% of its client population experiences symptoms of mental illnesses.”
The most common mental illnesses encountered within treatment and care sites include depression, anxiety, bipolar disorder and schizophrenia; substance use disorder is also common within the PLHIV client population. A key area of interest is the integration of the Collaborative Care Model into the already existing treatment and care system, in a manner that incorporates the unique features of each site. The Collaborative Care Model is an evidence-based approach to treating common mental health conditions (e.g., depression, anxiety) in primary care settings and was developed at the University of Washington.
I-TECH also assisted the NACC with the establishment of the National HIV Helpline and will continue to provide support over the next six months, while working to transition the program fully to NACC. This includes support for the HIV Helpline Coordinator and Active Listeners, as well as training of new Active Listeners.
“We must continue fighting the stigma associated with living with HIV,” says Conrad Mitchell, Program Coordinator. “It’s important to continue to battle misinformation and to have that coupled with positive true-life experiences. The Helpline–manned by persons living with HIV together, with HIV NGO advocates and allies–provides a unique opportunity to combat misinformation though empathy and education in direct, one-on-one engagements with the public.”
A 2017 Inter-American Development Bank (IDB) National Women’s Health Survey for Trinidad and Tobago[1] showed that more than 30 percent of women in Trinidad and Tobago had reported having experienced at least one incidence of either physical or sexual partner violence. The NACC is seeking support related to GBV and the risks it poses to the health and well-being of PLHIV. Activities would focus on raising awareness and providing resources and psychosocial support for vulnerable groups.
“There is a lack of general knowledge about GBV and what it entails among the public as well as in some health care settings,” says Ms. White. “There is an opportunity to yield enormously positive results by increasing the knowledge and insight of health care workers, and people living with HIV, regarding GBV.
“My hope is that the information that is shared empowers people living with HIV to advocate for themselves if they come to the realization that they are experiencing,” she continues, “and to make contact with the local resources that are available to receive the necessary support.”
On 18-19 May 2022, the International Training and Education Center for Health (I-TECH), in collaboration with the Programme National de Lutte Contre le Sida (PNLS; National AIDS Control Program) under the coordination of the General Directorate of Health, hosted its first national HIV prevention, care, and treatment quality improvement (QI) conference in Abidjan, Côte d’Ivoire. The conference brought together over 100 representatives from the Centers for Disease Control and Prevention, United States Agency for International Development, the Human Resources and Services Administration (HRSA), US President’s Emergency Plan for AIDS Relief (PEPFAR), and PEPFAR implementing partners from around the country to agree on a national approach to QI; update the national strategic plan for improving Quality, Health, and Safety; and learn about the unique QI approach being implemented by I-TECH through the Quality Improvement Solutions for Sustained Epidemic Control (QISSEC) program.
I-TECH QISSEC Project Director, Dr. Nathalie Krou Danho, describes the QISSEC approach at the National HIV QI Conference. Photo Credit: I-TECH
“This is an historic workshop. [There have been] many conversations and meetings with the PNLS/Ministry of Health and USG agencies [over the years] to gather all the stakeholders to harmonize QI interventions,” says Dr. Jean T. N’Guessan, QISSEC QI Consultant. “This national QI workshop was a success because the leadership was carried by the PNLS, the national Program to fight AIDS, and supported by I-TECH.”
The goal of the conference was to elevate QI practices on a national level and work with stakeholders to adopt and integrate the QISSEC QI approach into their own HIV prevention, care, and treatment programs to improve HIV services while identifying and addressing gaps in care (e.g., viral load monitoring, antiretroviral therapy uptake).
“In Côte d’Ivoire, all hospitals—both public and private—are required to implement continuous quality improvement for all care and services, which can lead to a one-size-fits-all approach to QI,” explains Dr. Nathalie Krou Danho, I-TECH QISSEC Project Director. “This workshop made it possible for us to identify gaps in national standards for the prevention, care, support, and treatment of HIV infection, while also providing an effective QI framework that helps clarify the roles and responsibilities of the stakeholders implementing QI initiatives across the country.”
QI interventions are often applied unilaterally across all sites regardless of analysis of the sites’ specific needs, but I-TECH’s approach tailors each QI intervention and related activities to the needs of the site according to self-identified gaps by the sites. This approach allows sites to be involved in each step of the process, reinforces skills and knowledge, and ultimately creates a sustainable approach to QI. By using the QISSEC approach, HIV programs around Côte d’Ivoire will be able to align their QI work and substantially improve HIV services, while also fulfilling PEPFAR priorities and targets.
“Since I-TECH’s approach works in collaboration with all levels (national, district, and site) of the health system pyramid, we are able to coach sites to develop a QI plan based on the identified gaps, implement it, as well as monitor and evaluate it,” says Dr. Nathalie Krou Danho. “Through data analysis of MER indicators and SIMS data, the approach takes into account the organizational improvement of the quality and the services offered to the patients.”
The QISSEC project, a five-year cooperative agreement with HRSA under PEPFAR, works with local partners to implement customized site-level QI interventions using patient-centered approaches in clinics to ensure a facility-owned and locally led response to the persistent challenges seen in HIV prevention, care, and treatment programs (e.g., HIV testing, retention, suppression, PrEP, TB prevention) and support Côte d’Ivoire in reaching the UNAIDS 95-95-95 targets. The project has initially been focused on 60 priority sites throughout the country but plans to expand to Abidjan’s 75 high-impact sites next year, bringing the total number of sites to 101.
“The QISSEC project aims to strengthen ownership of continuous QI at all levels of the health system pyramid,” says Dr. Nathalie Krou Danho. “To do this, I-TECH collaborates with all national stakeholders, including PEPFAR implementing partners and civil society organizations who can help motivate beneficiaries to take part in QI efforts and extend its QI approach to the community.”
I-TECH’S WORK IN CÔTE D’IVOIRE IS SUPPORTED BY THE HEALTH RESOURCES AND SERVICES ADMINISTRATION (HRSA) OF THE U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES (HHS) UNDER 1 U1NOA45176-01-00 THE CONTENT OF THIS POST IS THE AUTHOR’S AND SHOULD NOT BE CONSTRUED AS THE OFFICIAL POSITION OR POLICY OF, NOR SHOULD ANY ENDORSEMENTS BE INFERRED BY HRSA, HHS, OR THE U.S. GOVERNMENT.
A group of DREAMS ambassadors in Zimbabwe. Photo credit: Zim-TTECH
After facing incredible obstacles, three resilient 22-year-old women from Tsholotsho District, Zimbabwe, found their lives intersecting: Sitheni, Clemencia, and Faith are DREAMS ambassadors, equipping adolescent girls and young women with skills to reduce their vulnerability to contracting HIV–and helping them to find their own strengths.
DREAMS (Determined, Resilient, Empowered, AIDS-free, Mentored, and Safe) is a PEPFAR-funded program that aims to reduce HIV infections among adolescent girls and young women through not only prevention and treatment, but also a core curriculum that addresses HIV prevention, financial literacy, and gender-based violence (GBV). Participants can also access services such as HIV testing, family planning, pre-exposure prophylaxis (PrEP), counseling, and screening for GBV.
The International Training and Education Center for Health (I-TECH) has been supporting the Zimbabwe Technical Assistance, Training and Education Center for Health (Zim-TTECH) and its ZimPAAC consortium to implement the DREAMS program since 2020. To date, nearly 20,000 girls and young women in Zimbabwe have completed the primary DREAMS curriculum, Health for Life.
Sitheni, Clemencia, and Faith were initially enrolled in the DREAMS program as beneficiaries, having turned to transactional relationships (trading sex for money or necessities) to survive poverty amid the deepening economic crisis in Zimbabwe. They now use their own experiences to give back to young women who face similar choices.
Sitheni had to abandon her life-long goal of attending university to support her parents and four siblings; carrying the burden of sole provider for her family took a toll on her. When earnings from her part-time jobs weren’t enough, she became involved in sexual relationships with older, cross-border traders—known as omalayitsha—to make extra money.
Once enrolled in the DREAMS program, she thrived within the Health for Life courses, which cover financial literacy, social asset building, condom education, and violence and HIV prevention. “I encourage young girls in my community not to depend on men, but to use their skills instead of waiting to be given money by men who will abuse them,” Sitheni says.
Training and services are often provided in a safe space such as a school or community center, where participants meet with a mentor trained to deliver the Health for Life curriculum.
“At the moment I mentor 140 adolescent girls and young women aged 15-24 in the district,” says Faith, who also dated older men for money in order to make ends meet. “It is my duty to link adolescents with the district clinical nurse to access services at health facilities and safe spaces. I also encourage women to support people living with HIV/AIDS in the community. I teach them about human rights and encourage them to utilize their talents to make a living.”
Another part of Faith’s job is enrolling and following up on beneficiaries as well as supporting community-based facilitators who teach social asset building. This includes facilitating relationships and connections within DREAMS safe spaces to share encouragement and survival skills.
These safe spaces were critical to providing hope and new options for Clemencia. “After my father passed away, there was no one to pay for my school fees,” she says. “I came to my wits’ end, and I ended up exchanging sex for livelihood. At that time, it seemed the only viable option.”
Clemencia traded sex for two-and-a-half years, placing her among those at highest risk for HIV acquisition in Zimbabwe.[1] “Luckily for me, I did not get infected with HIV,” she says. “Ever since joining DREAMS, I have become empowered, and I know how to protect myself from sexual violence.”
Thanks to what she learned in her financial literacy sessions, Clemencia has started a small business of breeding hens and selling them to community members. “I also sell clothes for extra income,” says Clemencia, who now encourages other young women to complete their financial literacy sessions so they can start their own businesses and become independent.
Faith is thrilled to be able to foster this independence, as well. “Little did I know that I could make an honest living without anyone having expectations from me,” she says. “I am now able to encourage other girls and young women to stop engaging in transactional relationships. I am able to do this because I have been mentored and I have knowledge about HIV/AIDS and violence against women.”
[1] Chiyaka T, Mushati P, Hensen B et al. Reaching young women who sell sex: Methods and results of social mapping to describe and identify young women for DREAMS impact evaluation in Zimbabwe. PLoS One. 2018 Mar 15;13(3):e0194301. doi: 10.1371/journal.pone.0194301. eCollection 2018.
 Data from the International Training and Education Center for Health (I-TECH) program in Malawi were presented during the 2023 Conference on Retroviruses and Opportunistic Infections (CROI). The annual conference took place in Seattle, WA, from 19-22 February 2023, and brought together researchers, academics, and experts to discuss and present on their scientific achievements and new research.
Data from the International Training and Education Center for Health (I-TECH) program in Malawi were presented during the 2023 Conference on Retroviruses and Opportunistic Infections (CROI). The annual conference took place in Seattle, WA, from 19-22 February 2023, and brought together researchers, academics, and experts to discuss and present on their scientific achievements and new research.
 This story was first reported in
This story was first reported in 


