In March, the Botswana Ministry of Health and Wellness (MoHW), launched an online self-registration platform to allow eligible citizens to register for COVID-19 vaccination. The registration portal was developed by the International Training and Education Center for Health (I-TECH), in conjunction with the MoHW and the National COVID-19 Task Force. Since the launch, more than 60,000 people have registered for vaccination through the platform, and more than 45,000 people have received their first dose of the COVID-19 vaccine.
Screenshot of the COVID-19 registration portal
I-TECH assisted the MoHW to develop the following modules for the platform:
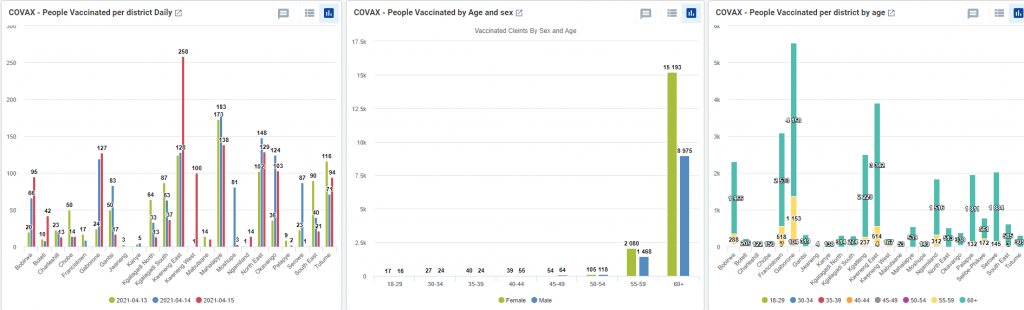
A DHIS2 tracker module tracks vaccinated clients for a follow-up dose. I-TECH trained MoHW health informatics and M&E officers to provide remote and on-site support to frontline health care workers across the country on application use. An interactive and intuitive dashboard shows vaccination trends across age and gender bands, geographical area and clinics/health facilities. The tracker module sends automated SMS reminders to clients regarding vaccination date, location, and time. Clients also receive a post-vaccination acknowledgment message.
An adverse events tracking module records any adverse events (AEs) due to COVID-19 vaccines. The module also automates reports on AEs and the correlation between AEs and any underlying conditions as disclosed by the clients.
A stock management module tracks the vaccine stock at facility, district, and national levels. This module is particularly helpful in projecting the vaccine demands at the clinics and vaccine availability against the vaccination bookings. The MoHW team closely monitors daily opening and closing stocks, to ensure optimal supply. Automated data checks and validations are built in to alert the facility management of any misappropriations in the vaccine stocks.
Available reports within the COVID-19 registration portal
Currently, I-TECH is working on a scheduling application that will be integrated into the portal for online booking of vaccination appointments. This will considerably reduce the number of “walk-in clients,” increase efficiency, and assist frontline workers in managing the workload at vaccination sites.
I-TECH will continue supporting this initiative until the end of the current funding cycle, while simultaneously capacitating the MoHW to take over the day-to-day management and maintenance of the portal.
This online, DHIS2-based platform is available here.
I-TECH’s work in Botswana is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under U91HA06801, the International AIDS Education and Training Center (IAETC). The content of this post is the authors’ and should not be construed as the official position or policy of, nor should any endorsements be inferred by, HRSA, HHS, or the U.S. government.
The International Training and Education Center for Health (I-TECH) is proud to support today’s launch of the World Health Organization (WHO) Global Strategy to Accelerate the Elimination of Cervical Cancer. I-TECH has supported interventions for education, testing, and treatment of cervical cancer since 2014.
In Namibia, I-TECH currently supports screening and treatment at 31 health facilities and 11 outreach sites in seven regions. As of August 2020, the program had performed more than 14,000 screenings and 1,700 treatment procedures for HIV-positive women.
The Namibia team has also launched a campaign to raise awareness of the importance of screening for and treatment of cervical pre-cancer in women aged 20–49. The campaign has been crucial during the COVID-19 pandemic, as patients may be less likely to visit their health care provider for preventive care, including cervical cancer screening and treatment.
I-TECH’s network partner in Botswana, the Botswana Training and Education Center for Health (B-TECH), will soon begin work on a national cervical cancer and treatment program, focused on women living with HIV. Activities will include providing quality routine cervical cancer screening and treatment for all eligible women living with HIV at high-volume ART sites in 12 districts, as well as raising awareness among this population.
B-TECH — in conjunction with I-TECH, University of Botswana, and the National Cervical Cancer Prevention Program (NCCPP) — will align national screening and treatment guidelines with WHO standards to ensure sustainability. B-TECH will also work closely with National Laboratories to increase capacity for quality cervical cancer screening services.
Dr. Linda Eckert, UW Professor of Obstetrics & Gynecology as well as Global Health, is lead coordinator for updating WHO recommendations on cervical cancer screening and treatment and serves as technical advisor to I-TECH in this work in Namibia and Botswana. She notes that the time has come for the WHO strategy.
“The WHO’s Cervical Cancer Elimination Strategy will literally save millions of women’s lives around the globe,” says Dr. Eckert. “Each year, over 300,000 women die of cervical cancer, and the number of deaths is projected to increase by over 20% in the next decade.
“Almost all cervical cancer can be prevented—making these deaths even more tragic,” she continues. “This is the first time WHO has launched a cancer elimination strategy, calling on the global community who care for women to say ‘enough’ to cervical cancer, ‘enough’ to these preventable deaths.”
The B-TECH team implements innovative, high-yield testing approaches to increase HIV case identification and yield.
On October 1, the International Training and Education Center for Health (I-TECH) celebrated the launch of the local and independent Botswana Training and Education Center for Health (B-TECH) and Caribbean Training and Education Center for Health (C-TECH).
For more than 17 years, these teams have worked within the regional Botswana and Caribbean offices of I-TECH to respond to the health needs of individuals and communities infected and affected by HIV. B-TECH and C-TECH, as locally registered non-governmental organizations, will continue to build on those years of experience implementing innovative, locally driven HIV prevention, care, and treatment programs, as well as expand their work to tackle other pressing health issues within the Batswana and Caribbean communities.
As part of the I-TECH network, B-TECH and C-TECH are able to access the academic depth and regulatory structures of UW and, together with local and regional clinical and programmatic expertise, scale up best practices and strengthen health systems. As local entities, B-TECH and C-TECH will also be able to take advantage of expanded partnership opportunities.
The C-TECH team also has broad experience with clinical mentoring at HIV treatment sites.
Both teams have supported pioneering work in their regions to provide comprehensive, patient-centered care for the most vulnerable populations. The C-TECH team has implemented a groundbreaking preceptorship program to improve provider communication with key populations affected by HIV in Jamaica and Trinidad and Tobago. It has also implemented a successful telementoring program through a Project ECHO®-based platform and model, reaching 465 providers. The program connects groups of providers to form communities of practice throughout the region to facilitate clinical updates, case consultations, and strengthened practice in HIV treatment and care and, recently, COVID-19.
“We look forward to remaining within the I-TECH family,” said Natalie Irving-Mattocks, Executive Director of C-TECH. “But our team is equipped and ready to move into this next chapter, deepening our local relationships, expanding our reach throughout the Caribbean, and building on our commitment to support access to high quality health care for the region’s most vulnerable.”
For its part, the B-TECH team has made an enormous impact on the health systems of Botswana, enabling the policy environment for HIV clinical case management; developing and implementing an interoperable, standards-based health information system; and enhancing the capacity of the health workforce at all levels. The team has also implemented innovative, high-yield testing approaches to increase HIV case identification. Targeted HIV testing strategies include partner testing services; HIV self-testing; testing among presumptive tuberculosis cases; and the expansion of afterhours and weekend testing to target men.
“We are excited to begin this new endeavor to promote innovative, locally driven, and effective programs to respond to the HIV epidemic in Botswana,” said Dr. Odirile Bakae, Executive Director of B-TECH. “With a high level of technical assistance from I-TECH, combined with B-TECH’s boots-on-the-ground approach, we are a winning team. We look forward to a fruitful partnership with both I-TECH/UW and the Government of Botswana.”
I-TECH has worked closely with UW Global Operations Support over the past decade to inform the internal procedures and structures necessary for international office registrations. This work has promoted operational effectiveness by enabling a safe, compliant, and legal environment for conducting international work. I-TECH’s close work with Global Operations Support has also helped to create the administrative and policy structures necessary to enable the successful launch of B-TECH and C-TECH.
Over the past two years, three other I-TECH offices – in Haiti, India, and Zimbabwe – have launched local organizations, signaling I-TECH’s bedrock commitment to transition, sustainability, and country ownership.
“These new organizations reflect our shared goals of serving communities, building capacity, and supporting expert leadership across the I-TECH network,” said Dr. Pamela Collins, I-TECH Executive Director. “We look forward to continued strong collaboration that saves lives.”
Read more about the B-TECH and C-TECH leadership teams below.
Dr. Odirile Bakae, Executive Director, B-TECH
Dr. Bakae is a physician with over 15 years of clinical experience in providing services to people living with HIV, as well as a deep understanding of structuring health programs to optimize client outcomes. He has several years of experience practicing medicine in public health settings in Botswana, including the management of the Infectious Disease Control Centers (IDCC), specializing in ART failure clients, complicated TB and HIV cases, and cervical cancer patients.
In addition to his role as B-TECH Executive Director, Dr. Bakae is the Principal Investigator for the CDC funded Cervical Cancer (GH20-2009) and Strategic Information Services (GH20-2007) awards.
He joined I-TECH Botswana in 2015 and led one of the most successful HIV testing programs in the country, focusing on a client-centered approach. Under his leadership, the country program performed exceptionally well, in terms of quality of service delivery and in meeting donor targets and expectations.
Ms. Kauta is a seasoned operations management professional with over 20 years of experience across a wide range of industries. She joined I-TECH Botswana in April 2009 and, as the Deputy Executive Director for B-TECH, she oversees operations, finance, and human resources, and is responsible for design and implementation of internal controls and compliance oversight at all levels of the organization.
In her management role, Ms. Kauta provides planning and coordination of efficient and effective support services to enable delivery of quality work to B-TECH clients and stakeholders. A key function of her role is to identify solutions to address operational challenges within B-TECH as well as ensure the implementation and adherence to the organization’s operational systems, policies and procedures.
Ms. Irving-Mattocks is a public health program director with extensive experience in managing projects focusing on health systems strengthening. She is also a business development practitioner with 13 years of experience in the field of social development. Her expertise includes financial management, budget management, project proposal writing, program design/development, planning, implementation and monitoring, strategic planning, and institutional development.
To her role as C-TECH Executive Director, Ms. Irving-Mattocks also brings deep experience and a proven track record in mobilizing and managing grants from international funding agencies such as United States Department of Human Services Health Resources and Services Administration (HRSA), PANCAP Global Fund, United States Agency for International Development (USAID), Clinton Foundation and National Institutes of Health (NIH).
Dr. Clive Anderson, Board Chair and Technical Advisor, C-TECH
Dr. Anderson has 30 years of experience as a primary care physician, specializing in HIV and STI care and prevention, as well as dermatology. He comes to his role as Board Chair and Technical Advisor after serving as Country Director of I-TECH Jamaica for the past three years.
He remains Technical Advisor to I-TECH Jamaica, where his experience also includes extensive experience as Technical Lead of the Caribbean Quality Improvement Collaborative (CareQIC), Lead HIV Project ECHO® Facilitator and Mentor, and clinical mentor at HIV treatment sites throughout Jamaica.
Dr. Anderson is currently a Clinical Assistant Professor in the Department of Global Health, University of Washington.
Dr. Ann Downer speaks at the I-TECH annual meeting in 2010.
On June 30, 2020, Dr. Ann Downer will retire from her post as the Executive Director of the International Training and Education Center for Health (I-TECH) at the University of Washington (UW).
Downer has had a 31-year career at UW; she founded I-TECH 18 years ago with a talented team of global health professionals at UW, along with her friend and colleague Dr. Michael Reyes, at the University of California, San Francisco. In that time, she has been the center’s trusted leader; a principal investigator for several awards; and a pioneering educator, mentor, and friend.
As is fitting for a hero’s journey, hers started on a boat.
After dropping out of University of California, Berkeley, as an undergraduate in the early ’70s, one semester shy of completing her degree, she worked as one of the only female commercial fisher-“men” in the Pacific Northwest for the lion’s share of her 20s.
Downer fishes in Neah Bay on the Makah Reservation in Washington, across the border from British Columbia.
“Mistake or not, [leaving UC Berkeley] set me on a path that school wasn’t setting for me at the time,” says Downer. “My experience fishing made me resilient, taught me how to work hard, and, above all, made me think about my future since I knew I couldn’t fish forever.”
But in order to finish school, she needed to set a new direction. On the advice of a female sailing instructor, she volunteered at Planned Parenthood Whatcom County in Bellingham, where she quickly secured a paying job.
“This one action — asking someone for advice — set my entire career in motion,” says Downer. “She prompted me to seek a new direction.
“And it was during my time as an education coordinator for Planned Parenthood that I gained the core skills that would serve me for the rest of my career,” she continues. “Teaching and instructional design, health education and curriculum development, comfort with discussing issues related to sexual health, and being in front of groups of people. Those years also solidified one of my core values — that people should have choice in regard to their own bodies.”
Downer finished her undergraduate degree while working at Planned Parenthood and then applied to the UW in Seattle. She went on to get a master’s degree in Health Education and Health Promotion at UW from a department (Kinesiology) that was later eliminated as duplicative with School of Public Health programs.
She again worked full-time during graduate school, exercising her entrepreneurial muscles helping to start a nonprofit program on prevention of child sexual abuse (the successful Committee for Children program has since expanded its work with parents and teachers to provide training on development of empathy and conflict resolution skills).
Downer and her team designed many of the first AIDS prevention campaigns in the state.
Following graduation and a year doing consulting work for clients such as the Washington State Office of the Superintendent of Public Instruction, Downer became the education coordinator in the mid-’80s for the first HIV/AIDS program at Public Health-Seattle and King County, where she and her team designed many of the first AIDS prevention campaigns in the state.
“I had learned by then that I really enjoyed working at the edge of emerging social issues,” she says.
Downer joined the UW faculty in the Department of Health Services in 1989. As a practice-focused educator working among researchers — and as a master’s-trained faculty member working closely with physicians, nurses, and PhDs — she had ample opportunity to call on the work ethic and tenacity she’d forged in the commercial fishing industry years earlier.
She eventually took the advice of her department chair, Dr. Bill Dowling, to continue her education. So, once again, she returned to school and worked full time while earning an advanced degree in educational leadership at Seattle University.
“The program wasn’t what I expected,” says Downer. “I thought it would concentrate on topics related to educational administration, like finance and law, but, while those topics were included in the curriculum, it was really a degree program focused on values-based leadership.
“I didn’t know it then,” she says, “but this was exactly what I needed in order to stay at UW and flourish.”
Values-based leadership became the foundation of two centers that Downer led at UW: the Center for Health Education and Research (CHER) and, later, I-TECH.
“I discovered that I could bring people together who shared certain values — respect for others, belief in the power of education, maintaining an attitude of hope, the desire to integrate practice and research,” she says. “These were the core values that guided us at CHER and carried over to I-TECH.”
CHER’s programs were initially focused on domestic public health challenges but began to expand in the direction of global health, so Downer approached Dr. Stephen Gloyd, who led the International Health Program (IHP).
“With Steve’s help and encouragement, we aligned more closely with IHP and began to grow our global portfolio of projects” says Downer. “As new projects were funded, the metamorphosis into what would become I-TECH was rapid, but our values and principles always remained the same.”
Downer and mentor Dr. King Holmes, Chair Emeritus of the UW Department of Global Health, in 2017.
I-TECH was formally founded in 2002 and moved from Health Services into the newly created Department of Global Health (DGH) in 2007, at the invitation of Dr. King Holmes, the founding chair of DGH. Holmes was closely involved in I-TECH from its inception and has been instrumental in its success; he remains a mentor to Downer and I-TECH to this day.
Since 2002, I-TECH’s cumulative funding at UW totals nearly $1 billion. I-TECH currently has an international staff of 2,000, with 13 offices in low- and middle-income countries, several of which have now transitioned to become independent, local organizations.
Downer was recognized by UW in 2015 as the recipient of the “Distinguished Contributions to Lifelong Learning” award, in part because of her growing interest in promoting e-learning at UW. Downer’s pioneering 12-week online course, Leadership and Management in Health, had graduated 25,242 participants as of March 2020, with an 87% completion rate. More recently, partnering again with the DGH e-Learning Program (eDGH) on a second 12-week professional development course, Project Management in Health, graduated 6,197 participants in its first two offerings, with a completion rate of 88%.
“My work with eDGH has brought me back to my roots in education,” says Downer, “designing educational products that include content and voices from diverse cultural traditions and perspectives. This is critical learning for those working in public health systems throughout the world — and especially important for improving the leadership and management skills of people working in those systems.”
I-TECH staff past and present, as well as assorted friends and family, gather virtually to toast Ann’s career and retirement.
Though officially retiring on June 30, Downer, as an emeritus professor in DGH, will continue to work for a small amount of time from July through December 2020 in order to finish one global health project under way in Cambodia and two online courses before turning them over to others.
At the same time, Downer does plan to be a retired person and reports that she’ll be busy in her garden, as always, and returning to her early roots as she again takes up sailing. Her adventure began — and now continues, it would appear — on the vast waters of our beautiful Pacific Northwest.
Downer is truly excited to see I-TECH move into the next phase of its organizational life under the leadership of Dr. Pamela Collins, Professor of Psychiatry and Behavioral Health, Professor of Global Health, and Director of the Global Mental Health Program.
“We all welcome you, Pamela!” says Downer. “I believe with all my heart that you are the right person at the right time for I-TECH. You inherit one of the most competent, resilient, and ethical groups of people you will ever work with — and a vision, mission and set of operating principles that I know are consistent with your own.
“I-TECH has been one of the loves of my life,” she continues, “and I wish you the same sense of fulfillment and pride I have had working with this incredible team of people — past and present — at this incredible university of ours.”
Dr. Pamela Collins, I-TECH’s new Executive Director
The International Training and Education Center for Health (I-TECH) is pleased and proud to welcome Dr. Pamela Collins as our new Executive Director, starting July 1, 2020.
A psychiatrist and mixed-methods researcher, Collins joined the University of Washington (UW) in 2018 as Director of the Global Mental Health Program, within the Department of Global Health (DGH) and the Department of Psychiatry and Behavioral Sciences. She also serves as Director of Faculty Development at DGH and as Principal Investigator of EQUIP Nairobi, a pilot implementation of Trauma-Focused Cognitive Behavioral Therapy (CBT) in Nairobi, Kenya.
Prior to arriving at the UW, Collins spent eight years at the National Institute of Mental Health, where she was Director of the Office for Research on Disparities & Global Mental Health and the Office of Rural Mental Health Research.
Collins was awarded an MD from Cornell University and an MPH from Columbia University, where she was a faculty member for 13 years. There, her research focused on the intersections of HIV prevention, care, and treatment and the mental health needs of women of color in the U.S., as well as diverse groups in Latin America and Sub-Saharan Africa. At Columbia, Collins was also the founding Director of the Global Health Track and Co-Director of the Initiative for Maximizing Student Diversity at the Mailman School of Public Health.
“I am humbled and thrilled by the opportunity to join and lead the I-TECH community,” says Collins, “as it applies its depth of experience and readiness for opportunity to a rapidly changing global health landscape.”
During the “Doctors for Justice” march on June 6, 2020, health care workers and others marched from Harborview Hospital to Seattle City Hall to protest police brutality.
Communities in the United States and globally continue to respond to the tragic murders of George Floyd and Breonna Taylor at the hands of police officers, as well as the death of Ahmaud Arbery, who was murdered by two White men, one of whom was a former police officer. We acknowledge the pain experienced by Black people and other communities of color. We acknowledge racism, police violence, and anti-Blackness as pervasive and systemic problems – and as barriers to the health and well-being of Black people and other communities of color. Racism and police violence are public health emergencies in the U.S., and we stand with Black communities in the fight against these public health and human rights violations.
Police violence against persons with black and brown skin is not new in the U.S. The United States were founded on racial violence – first through the mass destruction of indigenous communities and then again when the first ship bearing enslaved, captive Africans arrived in 1619. For hundreds of years enslaved people were bought and sold in the U.S. and, though slavery was officially abolished in 1865, the legacy of slavery lives on through the systemic racism, mass incarceration, and injustice that continue to impact our communities of color to this day.
I-TECH staffers and their families attend the “Doctors for Justice” march, which began outside of I-TECH headquarters.
I-TECH will continue to examine policies and procedures that foster safe workplaces for our colleagues of color, especially our Black colleagues; continuously examine and challenge our own biases; and strive to be purposely anti-racist in our actions. I-TECH remains committed to creating an environment where equity, diversity, and inclusion are core values and integral to our workplace and communities. We will hold ourselves accountable when those core values are not upheld.
Our thoughts are with Black members of the community, particularly the families of Mr. Floyd, Ms. Taylor, and Mr. Arbery and all of the other Black families who have lost loved ones to acts of racist violence. We will honor these individuals through our commitment to examining and reducing structural racism in our work.
If you would like to see how UW Health Sciences leadership have responded to these tragedies, read their message here.
Zim-TTECH staff supports Kowoyo Clinic in Goromonzi District, Mashonaland East Province, Zimbabwe. Photo credit: Macpherson Photographers.
The International Training and Education Center for Health (I-TECH) has transitioned another office to an autonomous entity. The Zimbabwe Technical Assistance, Training and Education Center for Health (Zim-TTECH) was officially launched on April 1, 2020, as a locally registered health trust. Zim-TTECH is the administrative and managing partner for the two existing I-TECH CDC/PEPFAR funded grants in Zimbabwe, each grant having a consortium of local partners:
ZimPAAC (Zimbabwe Partnership to Accelerate AIDS Control) is a partnership between Zim-TTECH, Africaid, Pangaea Zimbabwe AIDS Trust, and I-TECH. ZimPAAC collaborates with the Ministry of Health and Child Care (MoHCC) on context-appropriate health interventions to improve access to, as well as strengthen the quality of HIV prevention, treatment, care, and support services. ZimPAAC provides services at 373 facilities in 17 districts.
ZAZIC is a partnership between Zim-TTECH, I-TECH, and two local implementing partners—Zimbabwe Association of Church Related Hospitals (ZACH) and Zimbabwe Community Health Intervention Research Project (ZiCHIRe). ZAZIC supports voluntary medical male circumcision (VMMC) services at 38 static facilities in 13 districts.
“The transition from an I-TECH country office to a fully fledged independent local organization is exciting,” states Dr. Batsirai Makunike-Chikwinya, Zim-TTECH’s Executive Director. “Zim-TTECH is committed to continue to provide high-quality support to the MoHCC and to the health sector as a whole. Special thanks go to management and staff of both I-TECH/UW [University of Washington] and UZCHS-CTRC [University of Zimbabwe College of Health Sciences Clinical Trials Research Centre], who played pivotal roles during this transition.”
I-TECH has worked in Zimbabwe since 2003, collaborating with the MoHCC and other partners to improve clinical services and strengthen health systems. “It is a pleasure to support the launch of Zim-TTECH, which is the right next step toward country ownership and, importantly, recognizes the high level of skill and professionalism of the prior I-TECH country office and now Zim-TTECH team,” remarks Dr. Scott Barnhart.
Voluntary medical male circumcision (VMMC) safely reduces the risk of female-to-male HIV transmission by up to 60%. Few men have any post-operative VMMC complication. However, current practice in Zimbabwe and throughout most of sub-Saharan Africa requires VMMC patients to return for multiple, in-person post-operative visits. With low complication rates, and severe healthcare worker shortages, these required visits are a burden for providers and patients — threatening achievement of critical HIV prevention targets. A two-way texting model studied by University of Washington researchers in Zimbabwe offers a new way to address this barrier by reducing provider workload while also safeguarding patient safety.
“These visits can be a barrier to male circumcision uptake and expansion in countries with severe health care worker shortages, as well as negatively impacting patients who needlessly pay for transport, miss work, and wait for unnecessary reviews,” said Principal Investigator Caryl Feldacker, PhD, MPH, at the International Training and Education Center for Health (I-TECH) in the University of Washington Department of Global Health.
The study included 721 VMMC patients in two locations in urban Zimbabwe. In the study, patients communicated directly with a health care worker through interactive text messaging for the critical 13 days post-VMMC, rather than returning for required in-person visits. By giving men the option to heal safely at home, or return to care when desired or if complications arose, the method dramatically reduced in-person visits by 85%. Texting also reduced follow-up costs by about one-third while improving the quality of care.
As compared to routine in-person care, the study yielded twice the number of reported complications. “This increased identification and reporting is a positive result that is likely attributable to improved counseling and men’s engagement in care. Through texting, men were empowered to observe their healing and report potential issues promptly, before they worsened,” said Feldacker.
Currently, most text-based health care efforts blast pre-defined messages to many people simultaneously, removing patients’ ability to communicate back with health care workers. In contrast, two-way texting between providers and patients provides interactive care, and the short time frame heightened participation: in the study, 93% of men responded to texts. Both providers and clients reported confidence in the texting option, feeling safe and highly recommending it for scale.
“With the current system, Zimbabwe could perform millions of unnecessary follow-up visits over the coming five years. The workload burden for health care workers and time lost for patients who are healing without complication is a significant burden for health care workers and clients alike,” said Feldacker. “Potential gains in efficiency and reduced costs through using two-way messaging are large.”
With funding from the U.S. Centers for Disease Control and Prevention (CDC), and in partnership with the Society for Family Health, the model will soon be tested in urban South Africa. The new, field-based research will further test two-way texting in a different geographical and patient context to better inform the model for adaptation and widespread scale-up.
Feldacker added that “while our findings are grounded in studies on male circumcision, our results are largely attributable to the methods rather than to a specific disease or condition.
“With minimal adaptation,” she continued, “two-way texting could streamline other post-operative care contexts or be re-configured for other similarly acute, episodic conditions where continuity of care within a short period is critical for patients, such as short-course TB treatment, post-operative healing, post-natal care or early childhood illnesses — diarrhea, pneumonia, malaria — laying the foundation for generalizing to other diseases and contexts.”
For more on the study, see the paper pre-published in the Journal of Acquired Immune Deficiency Syndromes (JAIDS):
The study was led by Caryl Feldacker, and co-investigators are Vernon Murenje (International Training and Education Center for Health (I-TECH), Harare, Zimbabwe); Mufuta Tshimanga (Zimbabwe Community Health Intervention Project (ZiCHIRE), Harare, Zimbabwe); Scott Barnhart, Isaac Holeman, and Joseph B. Babigumira (Department of Global Health, University of Washington); Sinokuthemba Xaba (Ministry of Health and Child Care, Harare, Zimbabwe); and technology partner Medic Mobile (Nairobi, Kenya).
The Zimbabwe 2wT study was supported by the Fogarty International Center of the National Institutes of Health under Award Number R21TW010583.
Pictured are mannequins used at two regional training centers for nurses, midwives, and dental nurses in Kampong Cham and Battambang, Cambodia. I-TECH has supported the procurement of new mannequins to replace those that are old or broken, as well as new teaching tools that will expand the centers’ ability to conduct simulation training. Photo credit: Ann Downer/I-TECH.
The International Training and Education Center for Health (I-TECH) is working on a project led by FHI360, and funded by the U.S. Agency for International Development (USAID), to empower health care managers and national and provincial stakeholders to improve service quality, safety, and utilization, as well as strengthen overall health systems in Cambodia.
The project’s four objectives include:
Improving policies, guidelines and standards for streamlined quality assurance.
Increasing the efficiency and effectiveness of service delivery.
Strengthening regulatory framework, implementation, and enforcement.
Supporting pre-service public health training.
Given I-TECH’s deep experience in health workforce development, supporting the environments that enable strong health systems, and working with stakeholders at all levels, the team was a natural fit for Objectives 3 and 4.
In service of this critical work, I-TECH is supporting implementation of regulations among private and public health workers, as well as helping to lay the foundation for a sustainable accreditation program for public and private health facilities. I-TECH’s team also works with national stakeholders to develop the capacity of pre-service training institutions to deliver high-quality programs aligned with current evidence and national health priorities.
“We are excited to work with our partners to strengthen these critical components of quality health services in Cambodia,” said Jeff Lane, Principal Investigator and Assistant Professor in the Department of Global Health.
“By leveraging I-TECH’s broad experience in health policy, regulation, and workforce development,” he continued, “we can help Cambodia build an accreditation program to recognize high-performing hospitals, strengthen health professional councils to regulate health practitioners, and build sustainable pre-service training institutions that deliver competency-based education to train Cambodia’s health care workers of tomorrow.”
Participants of the national consultation on PBI model development discuss international best practices. Photo courtesy of I-TECH Ukraine.
In response to the need to quickly revitalize efforts to reach targets in Ukraine, CDC Ukraine has asked International Training and Education Center for Health (I-TECH) to support a performance-based incentive (PBI) model.
On March 28, 2019, I-TECH facilitated a high-level stakeholder workshop centered on PBI evidence and “best practices.” Participants from the U.S. Centers for Disease Control and Prevention (CDC) in Ukraine and the Public Health Center (PHC) of the Ministry of Health of Ukraine, and I-TECH gathered to discuss options for adapting proven methodologies to Ukraine’s HIV services.
PHC launched the model in December 2018 at five pilot sites across the country. In the pilot, monetary incentives were paid to individual doctors at the facilities to double efforts toward initiating new patients on ART.
PHC plans to expand the model to all 12 priority regions in the country. On the heels of COP ’19 discussions in South Africa, CDC Ukraine is looking for additional areas of the HIV cascade to which PBI could be applied to reach the FY2020 targets set by the U.S. Office of the Global AIDS Coordinator (OGAC).
The March meeting and the preceding preparatory meetings provided catalytic opportunities for identifying additional HIV services–including index partner testing, linkage to care, and loss-to-follow-up search–that could potentially benefit from the PBI model; discussing lessons learned from other PBI global initiatives; and utilizing evidence-based practices to design well-conceived and context-driven programs.
Marianne Holec, Senior Program Manager for I-TECH Zimbabwe’s voluntary medical male circumcision program; Efison Dhodho, Results-based Financing Health Specialist from the Programs Coordination Unit of the Ministry of Health of Zimbabwe; and Charbel El Bcheraoui, PhD, Assistant Professor at the Institute for Health Metrics and Evaluation (IHME) were keynote speakers at the event.
These working meetings resulted in meaningful exchanges between the guest speakers and Ukrainian experts about the successes (e.g., an increase in short-term achievement of targets and the opportunity to identify and target largest areas of need) and challenges (e.g., workplace friction, dissatisfaction with incentives, lack of teamwork, and reduced quality of care) of PBI implementation globally and in Ukraine to date.
Meeting participants appreciated the practical advice given by the guest speakers on designing effective, intentional, and sustainable PBI models for the longer term for HIV services. Experts advised developing a well-designed program that is adapted to local context; starting at a few sites and try different strategies to see what works best; gathering input from the providers as to what will work best; building in health competition between sites; and having a strong M&E framework.
With input from local stakeholders and international experts, I-TECH Ukraine has accepted the challenge of incorporating the key outcomes from the series of PBI meetings to structure the Ukrainian PBI model for HIV services. This narrative will include an outline of additional technical assistance required around its implementation.
THIS PROJECT IS SUPPORTED BY THE HEALTH RESOURCES AND SERVICES ADMINISTRATION (HRSA) OF THE U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES (HHS) UNDER U91HA06801, THE INTERNATIONAL AIDS EDUCATION AND TRAINING CENTER (IAETC). THE CONTENT OF THIS POST IS THE AUTHOR’S AND SHOULD NOT BE CONSTRUED AS THE OFFICIAL POSITION OR POLICY OF, NOR SHOULD ANY ENDORSEMENTS BE INFERRED BY HRSA, HHS OR THE U.S. GOVERNMENT.
 March, the Botswana Ministry of Health and Wellness (MoHW), launched an online self-registration platform to allow eligible citizens to register for COVID-19 vaccination. The registration portal was developed by the International Training and Education Center for Health (I-TECH), in conjunction with the MoHW and the National COVID-19 Task Force. Since the launch, more than 60,000 people have registered for vaccination through the platform, and more than 45,000 people have received their first dose of the COVID-19 vaccine.
March, the Botswana Ministry of Health and Wellness (MoHW), launched an online self-registration platform to allow eligible citizens to register for COVID-19 vaccination. The registration portal was developed by the International Training and Education Center for Health (I-TECH), in conjunction with the MoHW and the National COVID-19 Task Force. Since the launch, more than 60,000 people have registered for vaccination through the platform, and more than 45,000 people have received their first dose of the COVID-19 vaccine.